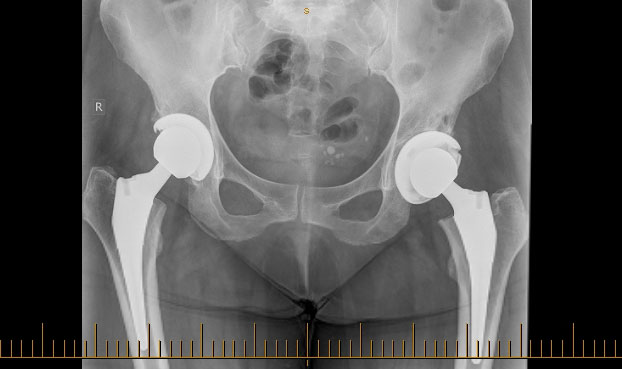
A total hip replacement is a surgical procedure in which the hip joint is replaced by a prosthetic implant.
Hip replacement becomes necessary when pain and deformity occur in the hip joint due to a variety of reasons, the most common of which is osteoarthritis.
Untreated arthritis of the hip joint is progressive causing severe disability, pain and ill health.
Hip replacement is now commonplace and in most instances patients are able to get back to almost all of their pre-arthritis activities
Dr Redgments results from the
National Joint Registry show that in his patients after 16 years more than 96% still have successful in place implants. This is compared to a national average of 92%.