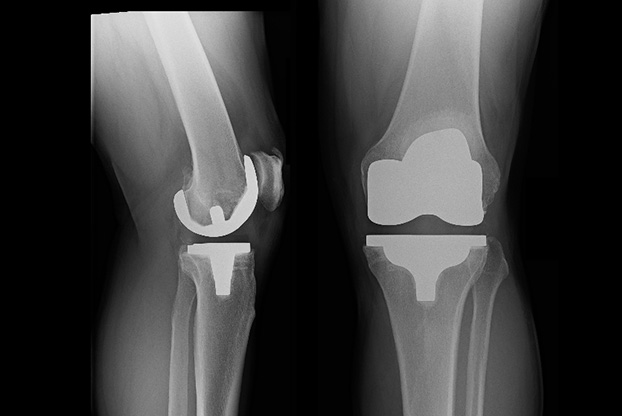
Total Knee Replacement is a surgical procedure in which the knee joint is replaced by a prosthetic implant.
Knee replacement becomes necessary when pain and deformity occur in the knee joint due to a variety of reasons, the most common of which is osteoarthritis.
Untreated arthritis of the knee joint is progressive but surgery is not recommended until symptoms interfere with daily activities or where pain occurs at rest or is associated with instability.
Knee replacement is now commonplace and in most instances patients are able to get back to almost all of their pre-arthritis activities.
Knee replacement surgery has continued to advance with the biggest change being the trend towards Kinematic or Functional Alignment. These advances mean:
Dr Redgment's results from the National Joint Registry show that in his patients after 19 years 96% still have successful in place implants. This is compared to a national average of 91%.
Dr Andrew Redgment (Wagga Wagga)
2 Foxborough Ave
Wagga Wagga NSW 2650
St Vincents Private Community Hospital Griffith
41-45 Animoo Avenue
Griffith NSW 2680